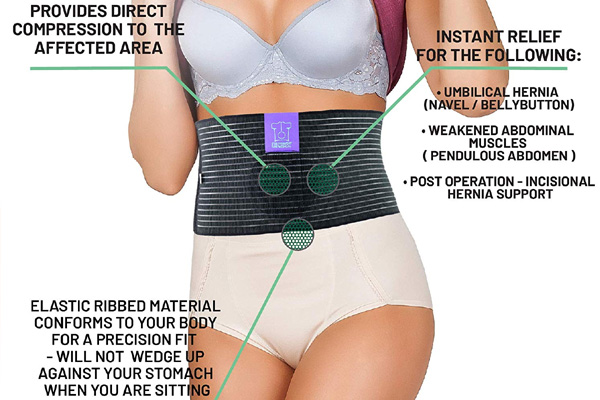
Umbilical Hernia Repair
It is also known as the exomphalos/ Omphalocele. It results from failure of part or all of the midgut to return to the coelom during early fetal life. It is classified as those that cause a fascial defect that is less than 4 cm (herniation of the umbilical cord) and those that has a fascial defect that is greater than 4cm.